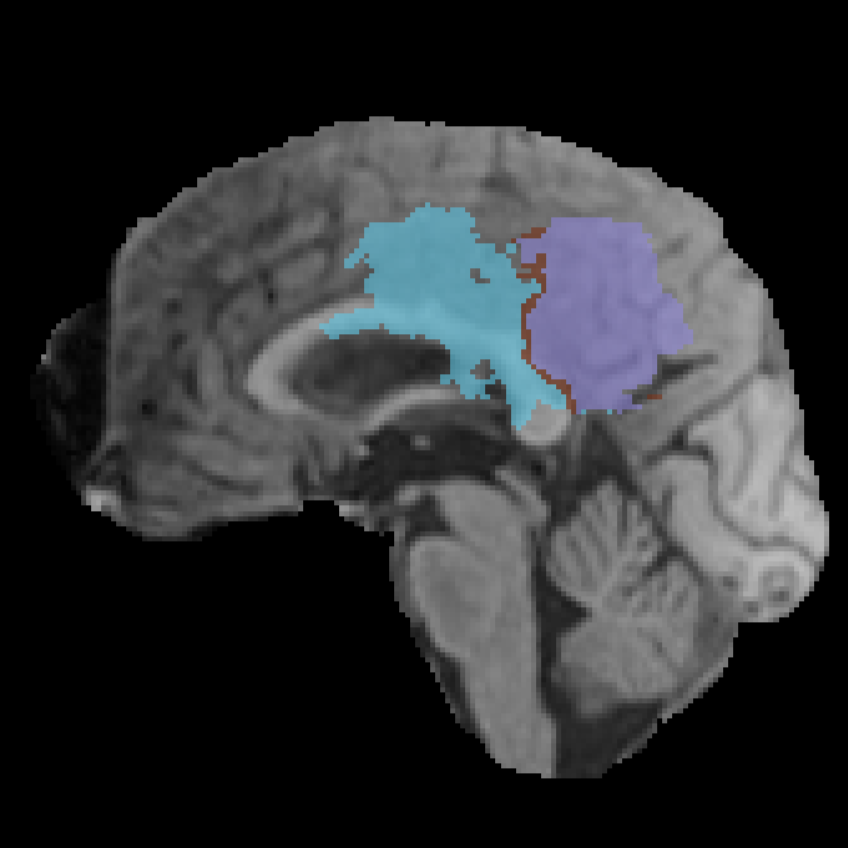
| F001 |
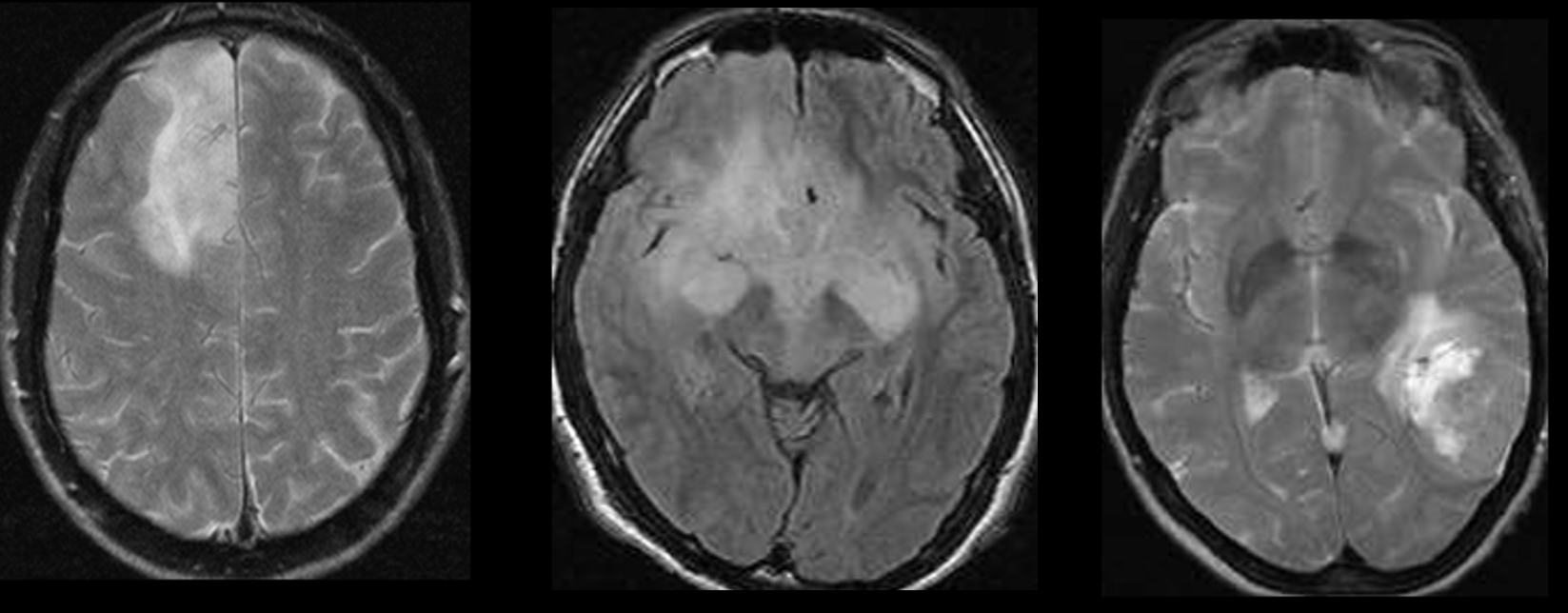
Tumor Center Region |
The tumor center is defined as the barycenter, or center of mass, of the TC region. The location of this point within the atlas is used to assign the corresponding anatomical region. To avoid cases in which the barycenter lies on a boundary, a spherical neighborhood with a radius equal to one tenth of the axial diameter is considered. The assigned region is then defined as the most prevalent region within this sphere. |
Machine |
| F002 |
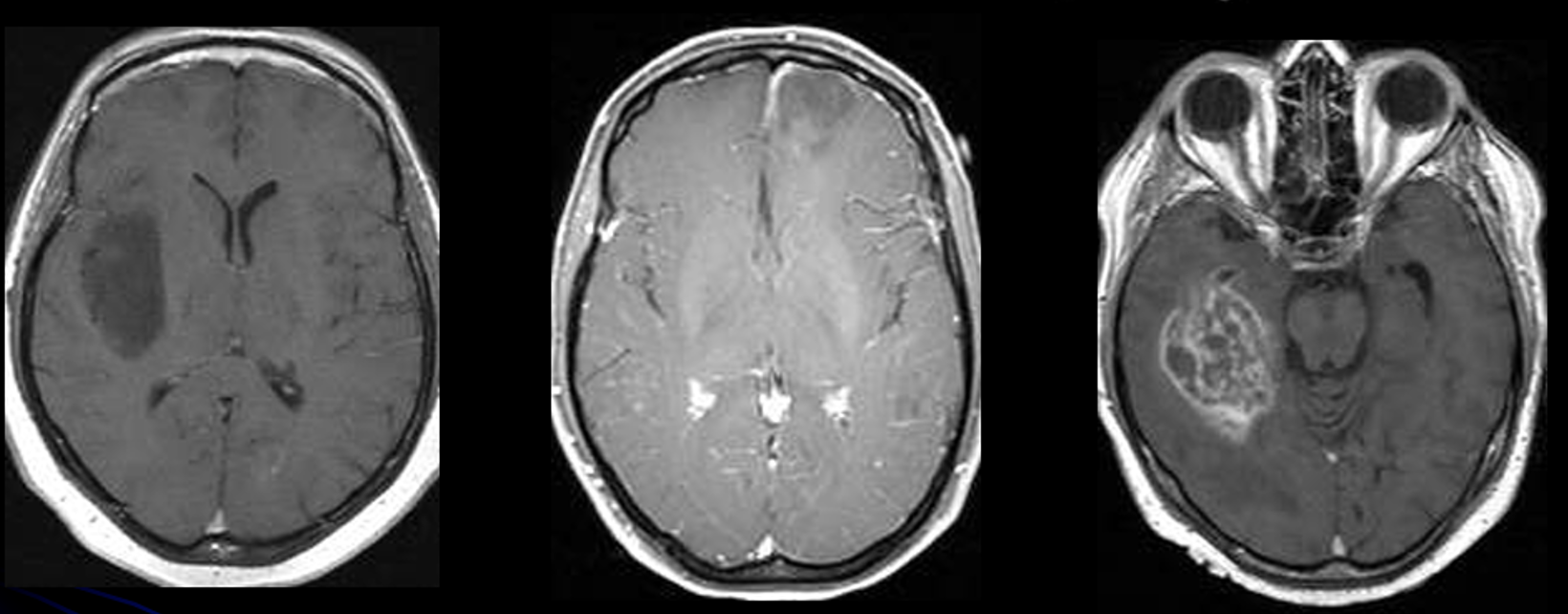
Tumor Center Coordinates |
The coordinates of the barycenter are computed as the mean coordinates of all voxels in the TC region. |
Machine |
| F003 |
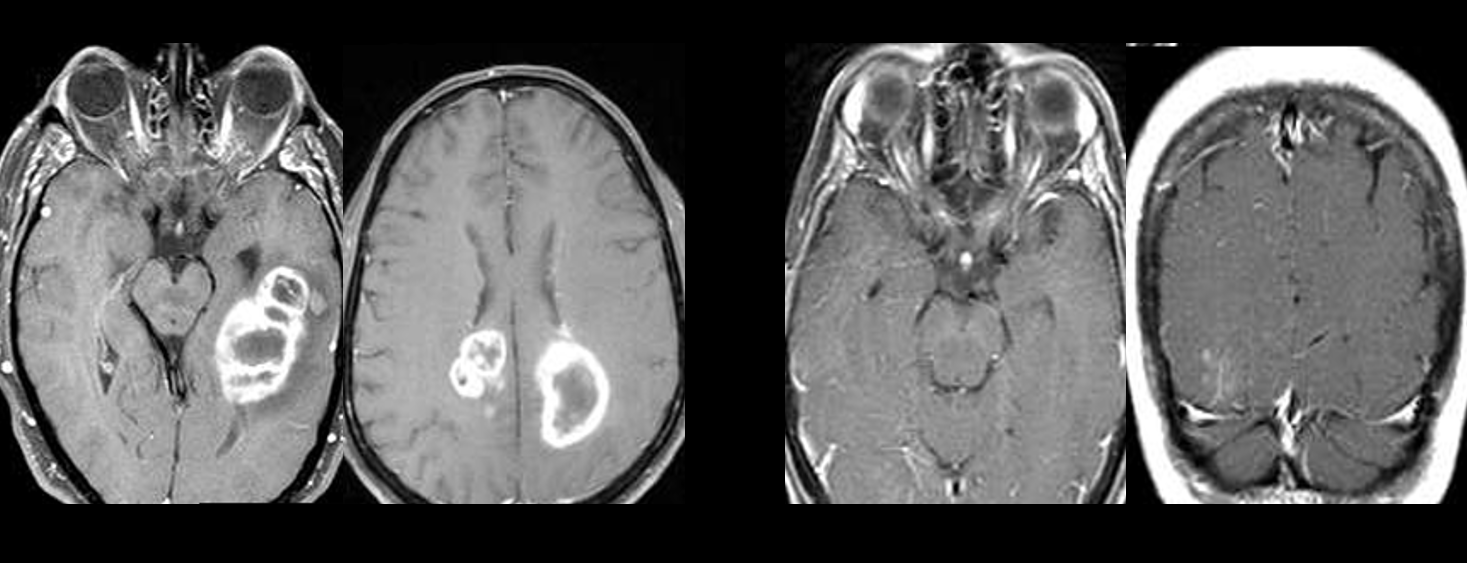
Side of Tumor Center |
Defined as the anatomical laterality of the tumor center based on the position of the TC barycenter relative to the brain midline, e.g., left, right, or midline. |
MachineAnnotator |
| F004 |
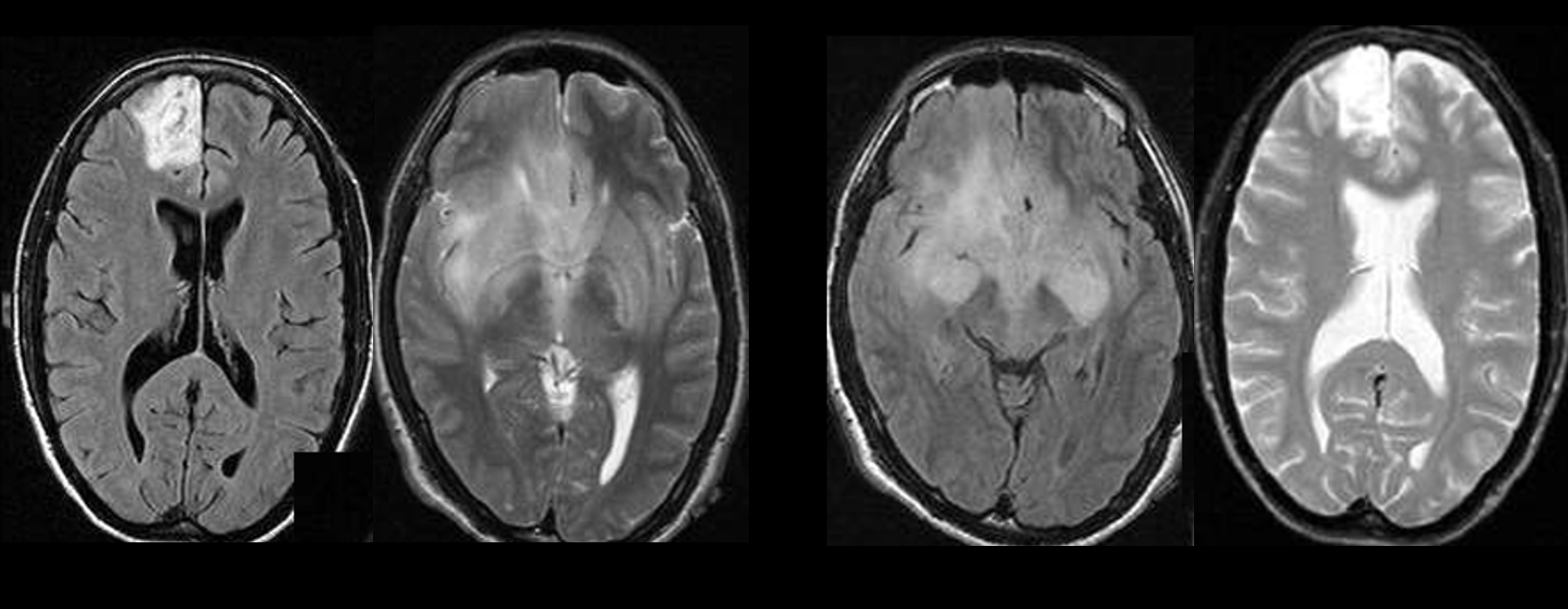
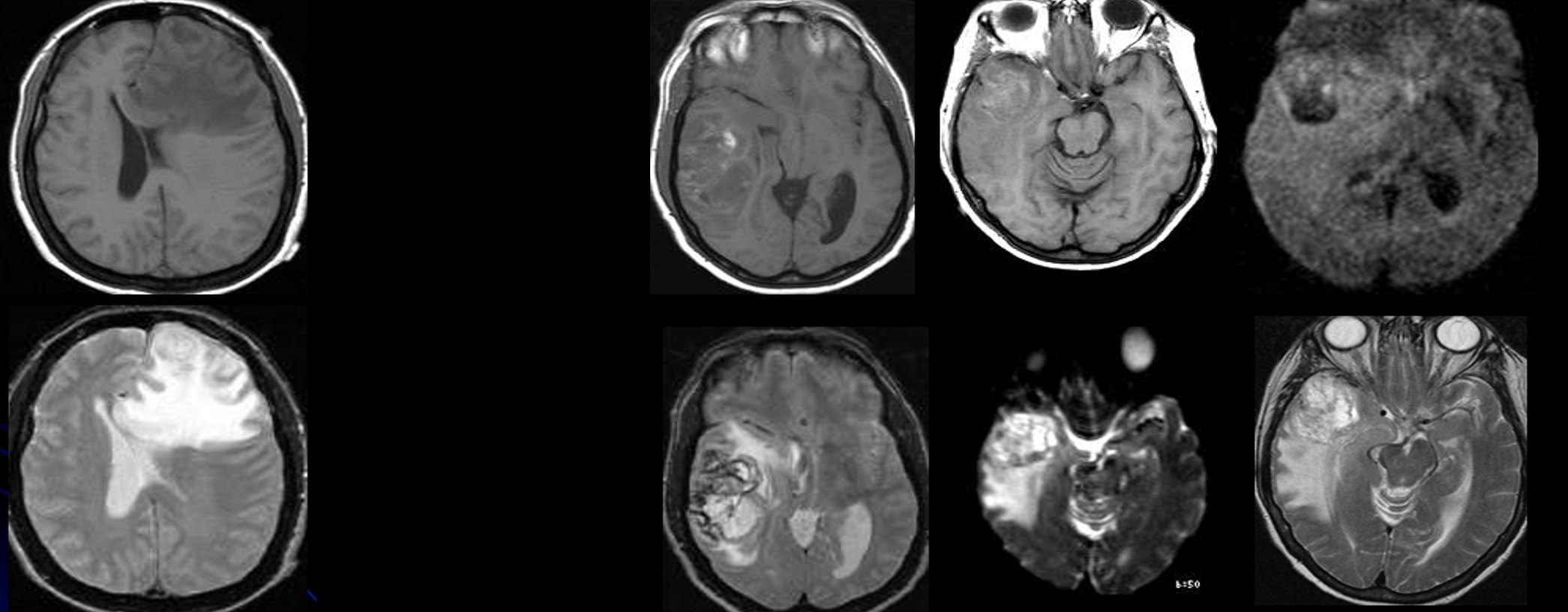
Eloquent Brain Involvement |
Determined using the atlas, this field specifies which of the following eloquent functional areas are involved by the tumor: vision, motor, speech motor, and speech receptive. |
Machine |
| F005 |
Enhancement Quality |
Qualitative assessment of CET contrast enhancement, indicating whether enhancement is present and how pronounced it appears. |
Annotator |
| F006 |
Proportion of ET |
Automatically derived from the segmentation mask using the formula: n. voxelET / n. voxelWT. |
Machine |
| F007 |
Proportion of ED |
Automatically derived from the segmentation mask using the formula: n. voxelED / n. voxelWT. |
Machine |
| F008 |
Proportion of NETC |
Automatically derived from the segmentation mask using the formula: n. voxelNETC / n. voxelWT. |
Machine |
| F009 |
Thickness of ET Margin |
Defined as the geometrically computed average thickness of the ET margin. |
Machine |
| F010 |
Definition of the Enhancing Margin |
Assesses whether most of the outer margin of the enhancement is well defined or poorly defined. |
Annotator |
| F011 |
Definition of the Non-Enhancing Margin |
Assesses whether most of the outer margin of the non-enhancing component is well defined or poorly defined. |
Annotator |
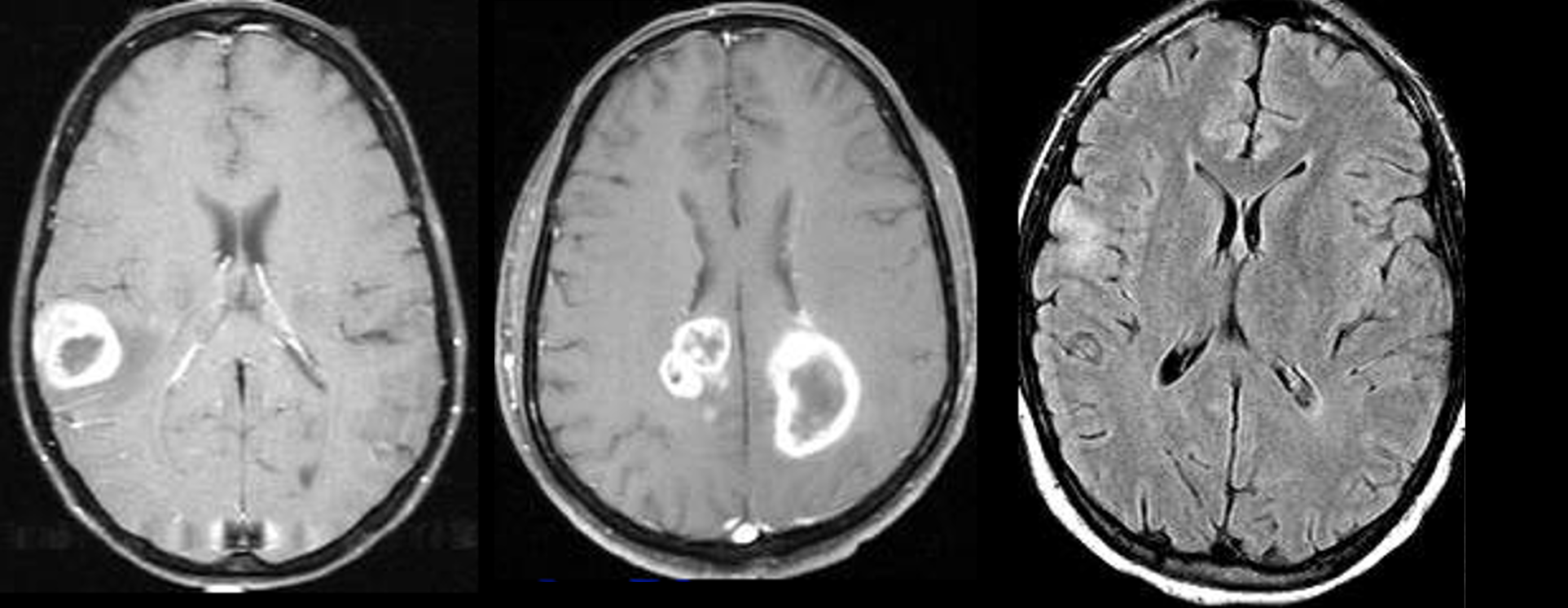
| F012 |
Intratumoral Hemorrhage |
Assesses whether intrinsic hemorrhage is visible anywhere in the tumor matrix. |
Annotator |
| F013 |
TC Size |
Defined as the largest perpendicular cross-sectional diameters of the TC across the axial, sagittal, and coronal planes. |
Machine |
| F014 |
ED Size |
Defined as the largest perpendicular cross-sectional diameters of the ED across the axial, sagittal, and coronal planes. |
Machine |
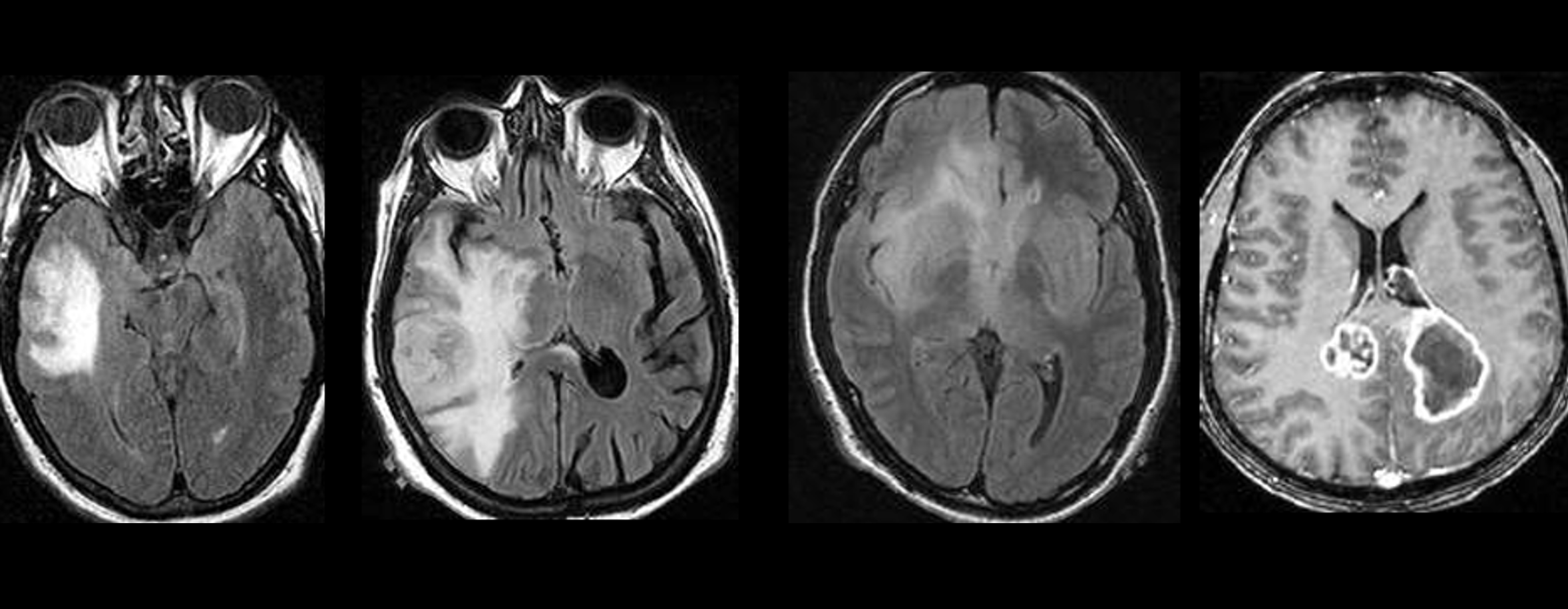
| F015 |
Tumor Heterogeneity |
The degree of heterogeneity of the internal architecture of the tumor. |
Annotator |
| F016 |
TC Affected Areas |
Determined using the atlas, this field specifies which brain regions are affected by the TC. |
Machine |
| F017 |
ED Affected Areas |
Determined using the atlas, this field specifies which brain regions are affected by the ED. |
Machine |
| F018 |
Number of Lesions |
Number of independent lesions observed in the brain. |
MachineAnnotator |
| F019 |
Type of Lesion |
Categorical variable indicating the observed lesion type. Possible values: single, multicentric, or multifocal. |
MachineAnnotator |
| F020 |
Ependymal Invasion |
Assesses whether the TC abuts any adjacent ependymal surface. |
Annotator |
| F021 |
Depth of TC |
Determines the depth of the TC. Possible values: cortical, subcortical white matter, deep white matter and basal nuclei. |
MachineAnnotator |
| F022 |
Tumor Center Macroarea |
The macroarea, or lobe, in which the barycenter lies, obtained using the atlas. |
MachineAnnotator |
| F023 |
Midline Shift |
The shift of the midline caused by the tumor mass, in millimeters. |
Annotator |
| F024 |
Tumor Shape |
The approximate shape of the tumor mass. |
Annotator |
| F025 |
Tumor Origin |
Where the tumor originates, following the grades: Periventricular, Gyral, or Deep white matter. |
Annotator |
| F026 |
Tumor Crosses Midline |
State whether the tumor crosses the midline. |
Annotator |
| F027 |
Subject specific findings |
Any subject specific findings that do not fall under any predefined category. |
Annotator |